Many patients present themselves to
Braverman Reproductive Immunology with a history of
multiple failed IVF
cycles or
recurrent pregnancy losses and what many of these patients have in common are extremely low AMH levels
(AMH < 1).
The
average number of failed IVF
cycles prior to our care, in our low AMH patients is
3.6!
Once they have failed this number of cycles at the initial IVF centers,
many are told they need donor egg and are most likely in early Menopause.
What most of these centers failed to realize is that a
low AMH in young women under 40 is most often due to
Endometriosis (90% in our data), and if the diagnosis is not already known, many of
these cases are
Silent Endometriosis, patients who do not have any of the normal symptoms of endometriosis (Silent Endometriosis (diagnosis based on immune findings without typical
symptoms): high incidence in patients with repetitive IVF failures and
Miscarriage) and the diagnosis of endometriosis is not made until they present to
our clinic.
We make the diagnosis based on clinical history, family history, immune
testing, AMH, and sonogram data.
The poor egg and embryo quality associated with low AMH is caused by a
treatable inflammatory environment that damages the Mitochondria of the
eggs during development on each given cycle.
(Mitochondrial dysfunction and Correctible Reoccurring Aneuploid Conversion
Syndrome (CRACS) A new category of treatable recurrent miscarriages common
in Endometriosis and PCOS patients).
This
can be corrected with treatment and while egg numbers may remain low, patients have been
able to produce better quality eggs that lead to more successful pregnancies (Egg Mitochondrial Restoration Program - Treatment for those with egg quality
issues caused by Endometriosis and PCOS (Correctable Recurrent Aneuploid
Conversion Syndrome)).
It is important to note that
PGD/PGS testing does not resolve this problem as many times the genetic testing will be normal in these patients (as
it is the mitochondria, not the nucleus that is defective), and
when PGS/PGD testing is abnormal the
incorrect conclusion is again reached that the eggs are not good and the patient is wrongly
advised to have egg donation (Correctible Reoccurring Aneuploid Conversion Syndrome (CRACS) 79% had a
successful pregnancy with BRI A Review of 155 cases).
When most centers are not sure how to treat the IVF failures they turn
to PGD/PGS we do not recommend this.
Our data presented here, based on our
markedly high pregnancy success rates, suggests that poor egg quality associated with low AMH in endometriosis
patients is
correctable and these patients with low AMH that have failed more than 3 IVF cycles
should not be told they are in
Menopause or that they
need egg donation until they have had and failed our proposed therapies.
1. Our pregnancy success rates
-
An astoundingly high successful pregnancy rate among all age groups in our low AMH patients (Figure 1 and 2).
All our data is “highly” significant. Low p value. See our
Graphs at end of this review.
- <35: 78% (overall),
48% (per cycle)
-
36-40: 69% (overall),
52% (per cycle)
-
>40: 22% (overall),
11.5% (per cycle)
These patients:
- failed on average 3.6 IVF cycles prior to our care
- 88% were found to have endometriosis confirmed by laparoscopy (Figure 3).
- have an AMH <1 (including all patients with very low AMH < .1)
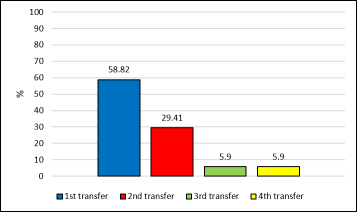
- 88% of the successes were within 2 IVF cycles with us (Figure 4).
- We did not routinely use PGS/PGD for these patients (an unnecessary and
a unneeded expense).
-
All success rates were
significantly higher than those reported in the literature for similar patients. These other
studies required up to 6 IVF cycles and did not approach our success rates
(Figure 1, 6, 7, 8).
-
88% of our patients that were successful did so within
just 2 IVF cycles accounting for the significantly higher per cycle success rates that we
report in addition to the high overall success rates.
These studies did not account for the complicated case load that we have
here at BRI as
our patients failed on average 3.6 IVF cycles prior to our therapies!
2. Our Data shows that:
- All patients with low AMH and a history of IVF failure should have a laparoscopy
(88% of our patients with low AMH had biopsy proven endometriosis).
-
The myth that surgery can harm your chances of successfully being pregnant
is likely wrong.
3.
Our treatment program
4.
Our data: Figures and statistics
-
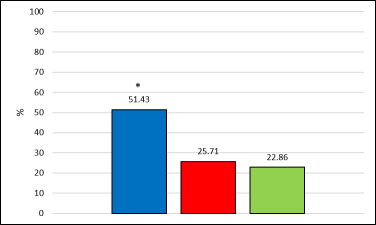
Figure 1: Overall BRI pregnancy success rate in AMH<1 patients based on their
age. Different letters mean that the difference is statistically significant
(**, p <0.01).
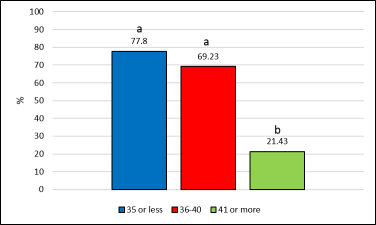
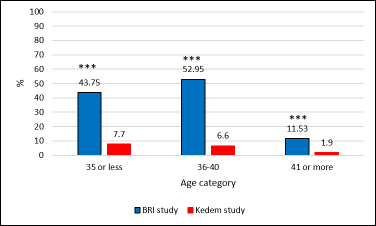
In our study, younger patients have better pregnancy success rate
per
cycle. Our rates
per cycle are up to 8-times higher than the ones reported in Kedem’s study
depending on the age category (***, p<0.001).
-
Figure 3: BRI patients with low AMH levels (< 1ng/mL) that were found to have
biopsy proven endometriosis.
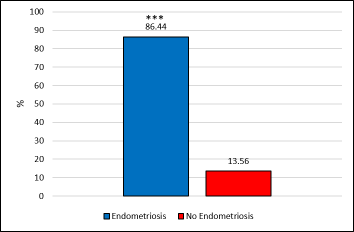
In patients with low AMH that underwent surgical laparoscopy, we found
86.44% of cases that had biopsy consistent with endometriosis (Figure
3, ***, p<0.001).
-
Figure 4: Pregnancy success rate in BRI patients with low AMH levels (< 1ng/mL)
based on the number of IVF transfers it took to be successful.
-
Figure 5: Pregnancy success in BRI patients with low AMH levels (< 1ng/mL) and
biopsy proven endometriosis that was excised (pregnancy success in blue,
loss in red, failed-ET in green, *:p<.05).
Success rates were even higher when patients were found to have endometriosis
and it was excised.
-
Figure 6: Comparison of pregnancy success rate (per patient not per cycle), this
includes even those patients in whom we did not find Endometriosis (only
12% of our low AMH patients) at BRI with several other studies in patients
with low AMH levels (< 1-1.2 ng/mL).
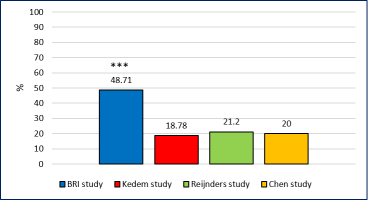
Many studies investigated the relation between IVF outcome and low AMH levels.
In these studies (1-3), the authors looked at patients with low AMH levels
(<1-1.2ng/mL) and reported a pregnancy success rate of 20% while we
are reaching 46.34% (***, p<.001). This number is highly significant.
Please note that we achieved our pregnancy success rate within 2 cycles
while the other studies took up to 6 cycles to achieve their low rates!
-
Figure 7: Comparison of cumulative pregnancy rate between BRI and Kedem’s
study in AMH<1 patients.
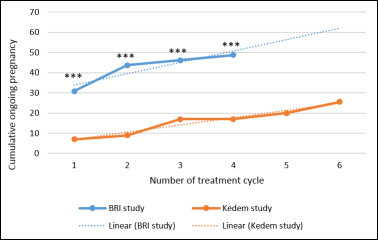
We are able to achieve a successful pregnancy within 2 IVF transfers in
the majority of our cases while Kedem’s group achieved a 20% pregnancy
success rate within 6 cycles (Figure 7, ***: p<.001).
-
Figure 8: Comparison of pregnancy success between BRI and Kedem’s study in
low (0.21-1 ng/mL) or extremely low (<0.2 ng/mL) AMH patient.
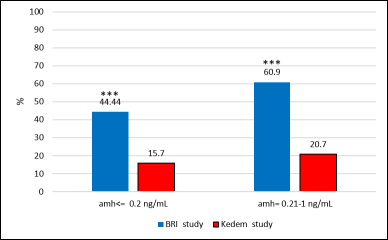
Kedem and collaborators showed no differences in the pregnancy rates between
patient with extremely low (<0.2 ng/mL) or low AMH levels (0.21-1 ng/mL).
Our study confirmed these findings although the pregnancy rate under our
care is significantly higher (3 times higher) regardless of AMH levels
(low or extremely low) as seen in Figure 8 (***, p<0.001).
References
- Kedem A, Haas J, Geva LL, Yerushalmi G, Gilboa Y, Kanety H, Hanochi M,
Maman E, Hourvitz A. Ongoing pregnancy rates in women with low and extremely
low AMH levels. A multivariate analysis of 769 cycles. PLoS One. 2013
Dec 16;8(12): e81629.
- Chen YP, Wu WH, Wu HM, Chen CK, Wang HS, Huang HY. Effects of anti-Müllerian
hormone and follicle stimulating hormone levels on in vitro fertilization
pregnancy rate. Taiwan J Obstet Gynecol. 2014 Sep;53(3):313-6.
- Reijnders IF, Nelen WL, IntHout J, van Herwaarden AE, Braat DD, Fleischer
K.The value of Anti-Müllerian hormone in low and extremely low ovarian
reserve in relation to live birth after in vitro fertilization. Eur J
Obstet Gynecol Reprod Biol. 2016 May;200:45-50.