Success Rates
After 30 years as a Reproductive Endocrinologist, Dr. Andrea Vidali understands the crucial role Endometriosis can play as an underlying condition causing multiple failures and pregnancy losses. Dr. Vidali has learned that for many patients, the missing link is not more testing — it’s a thorough surgical evaluation. Through expert excision of Endometriosis or correction of structural abnormalities, we’ve helped women who previously suffered repeated pregnancy losses achieve great success carrying healthy pregnancies to term.
As such, BRI/ESSI has evolved to become an Exclusive Endometriosis Treatment Center addressing the need for a hands-on and personal approach for the diagnosis and treatment of Endometriosis and the role it plays in infertility. While we no longer offer immunological testing or treatment services, our experience in this field continues to guide our understanding of the hidden drivers behind reproductive challenges. In particular, we have seen time and again how underlying conditions such as Endometriosis and Adenomyosis — often inflammatory in nature — play a critical role in reproductive failure and frequently go undiagnosed without surgery.
Historical Results from Our Legacy Program
In 2015, Dr. Jeffrey Braverman reviewed 30 cases at Braverman Reproductive Immunology & Endometriosis Surgical Center (BRI), demonstrating remarkable success among patients with five or more prior miscarriages. Of these patients, 80% achieved a successful pregnancy — defined as either a live birth or an ongoing pregnancy past 20 weeks (p<.0003, highly significant).
All documented losses were aneuploid (abnormal), showing that treatments were highly effective in maintaining euploid (chromosomally normal) pregnancies.
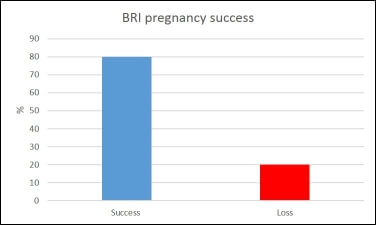 Figure 1: Overall pregnancy success at Braverman Reproductive Immunology showing approximately 80% success vs. 20% loss rate.
Figure 1: Overall pregnancy success at Braverman Reproductive Immunology showing approximately 80% success vs. 20% loss rate.
Pregnancy outcomes were consistent across different infertility categories — primary, secondary, and tertiary — meaning prior pregnancy history did not significantly affect success rates.
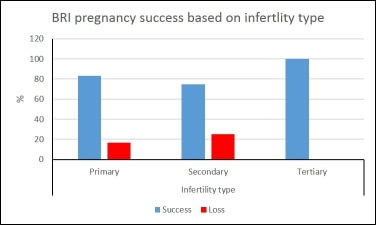 Figure 2: Success rates were consistent across infertility types: primary, secondary, and tertiary all exceeded 70% success.
Figure 2: Success rates were consistent across infertility types: primary, secondary, and tertiary all exceeded 70% success.
First Attempt Success Rates
When considering only the first attempt to conceive under our care, 60% of patients achieved success, with 83.4% of cycles performed using the patient’s own oocytes. For those using donor eggs, 80% conceived on the first attempt.
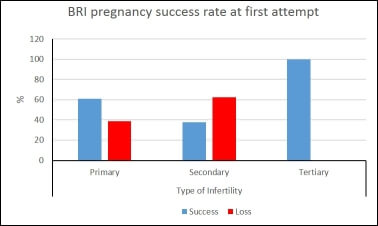 Figure 3: Success rate by infertility type for first attempt, showing consistent outcomes across primary, secondary, and tertiary infertility groups.
Figure 3: Success rate by infertility type for first attempt, showing consistent outcomes across primary, secondary, and tertiary infertility groups.
These findings demonstrate that, with appropriate therapy, women with multiple miscarriages — even those using donor eggs — can achieve normal, sustained pregnancies.
Understanding the Science Behind Recurrent Miscarriage
Research shows that miscarriage recurrence risk depends on genetic and immunologic factors:
- Women with prior euploid (normal genetic) losses face higher recurrence risk without treatment.
- Those with aneuploid (abnormal genetic) losses typically do not face increased risk for future miscarriages.
- Losses following a detected fetal heartbeat are more likely to be euploid and predictive of immune-related recurrence.
Comparative Research
Several landmark studies have shaped our understanding of recurrent miscarriage:
- Brigham Study (1999): Excluded many immune and endocrine factors (Endometriosis, PCOS, autoimmune disease), overestimating success rates because most included patients had aneuploid losses.
- Ogasawara Study (2000): Found that 49% of recurrent pregnancy loss (RPL) patients achieved success with treatment, but 80% of BRI patients did so using refined immunologic protocols.
- Morikawa & Carp Studies: Confirmed that recurrent miscarriage patients are more likely to lose euploid embryos — a pattern that demands immune-modulating treatment rather than observation.
Key Findings from Braverman Reproductive Immunology
- 80% overall pregnancy success in patients with 5+ prior miscarriages
- 60% first-attempt success rate with individualized immune therapy
- All recorded losses were aneuploid, confirming efficacy of treatment in maintaining normal pregnancies
- Inclusive patient selection — unlike prior studies, we included those with autoimmune disease, Endometriosis, and PCOS
Scientific References
- Brigham SA, Conlon C, Farquharson RG. A longitudinal study of pregnancy outcome following idiopathic recurrent miscarriage. Hum Reprod. 1999.
- Ogasawara M, Aoki K, Okada S, Suzumori K. Embryonic karyotype of abortuses in relation to the number of previous miscarriages. Fertil Steril. 2000.
- Morikawa M, Yamada H, et al. Embryo loss pattern in miscarriages with normal karyotype among women with repeated miscarriage. Hum Reprod. 2004.
- Carp H, Toder V, et al. Karyotype of the abortus in recurrent miscarriage. Fertil Steril. 2001.
The ESSI Difference: A Path Forward
If you have experienced:
- Recurrent miscarriage
- Multiple failed IVF cycles
- “Unexplained” infertility
- Or a family history of autoimmune/inflammatory disease
…then the next step may not be another lab test, but rather a thorough surgical evaluation with our team at ESSI.
We believe patients deserve more than vague answers like “bad luck.” Our center provides a clear, strategic path built on science, precision surgery, and compassionate care.
Request a Consultation today to learn whether surgical intervention could provide the answers and outcomes you’ve been seeking.