92% of conceptions have
a baby with our treatment protocol.
A Review of 48 cases at Braverman Reproductive Immunology
Another category of patients that seek our services are those that have
tried IVF and have had repetitive failed embryo transfers (ET). The
implantation process requires a complex and fine-tuned
cross-talk between thematernal and fetal side involving immune factors. The main factors for success appear to be the
embryo quality and the uterine environment, both appear to be important
for this immunologic cross talk.
We selected all patients with a history of repetitive failed IVF cycles
prior to our care that conceived under our care either on their own or
through IVF. This population consists of 2 groups of patients.
1.
Those that never conceived even prior to their multiple failed embryo transfer (40 out of 48 patients
never had a positive pregnancy test prior to our care) that we will group
under the term
primary infertility.
2. Those that did conceive prior to their repetitive failed embryo transfers. (8 out of 48). They
either had an early loss (5 out of 8) or a live birth (3 out of 8), we
will place this group under the term
secondary infertility.
All of our patients underwent full immune screening panel.
First results of our retrospective study based on 48 cases showed an overall
pregnancy success of
92%
among the patients who had repetitive failed embryo transfer prior to our
care and who did conceive after treatment with us (Figure 1). Pregnancy success is defined by a live birth or an ongoing
pregnancy past 12 weeks (p=.0001, a very low p value shows a very high
statistical significance).
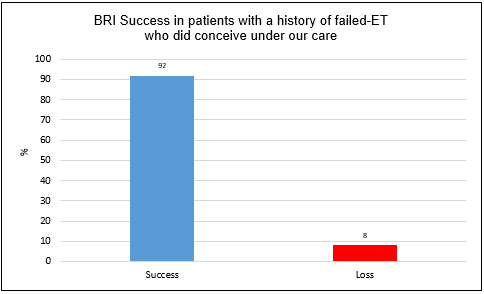
Figure 1: Pregnancy success at Braverman Reproductive Immunology in women
with a history of failed-ET prior to our care, who did conceive under
our care after adequate immune therapies (this is not a guarantee of future
performance).
There was
no significant difference between the different types of infertility as shown in Figure 2.
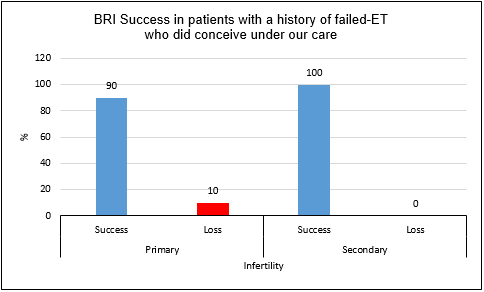
Figure 2: Pregnancy success rate at Braverman Reproductive Immunology based
on the type of infertility in women with a history of failed-ET prior
to our care and who did conceive under our care after adequate therapies.
With their first conception under our care,
81.25% of patients
had a successful pregnancy as seen in Figure 3 (p=.0001, a very low p value shows a very high statistical
significance).
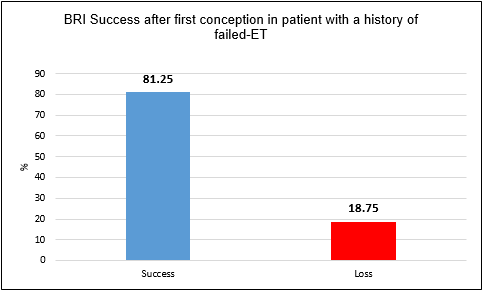
Figure 3: Pregnancy success rate at Braverman Reproductive Immunology at
first attempt in women with a history of failed-ET prior to our care,
who did conceive under our care after adequate therapies.
Patient age directly impacts egg/embryo quality and it is now largely accepted
that egg quality in addition to egg abundance significantly decreases
after the age of 35.
Based on demographic evidence (average age of our patient population is
36 years old with 58% of our patients being 35 or younger), it was obvious
that age alone could not explain the poor egg quality of our patients
(a finding of many of our patients prior to our care).
Endometriosis and polycystic ovarian syndrome (PCOS) are two conditions
that dramatically and negatively impact egg quality as well as egg number
(ovarian reserve), leading to genetically abnormal embryo (aneuploidy)
or embryos too “weak” to develop normally.
The increase in serum and peritoneal inflammation that is a result of PCOS
and endometriosis disrupts mitochondrial function and leads to poor embryo
development and behavior (for more information, read our blog entitled
“Mitochondrial dysfunction and Correctible Reoccurring Aneuploid
Conversion Syndrome (CRACS) A new category of treatable recurrent miscarriages
common in Endometriosis and PCOS patients“),
these two conditions are also responsible for failed-ET as well as the
miscarriages we have already reviewed in other blogs. This as well can
be treated leading to better egg/embryo quality and behavior and along
with treatment for the underlying immune issues also leads to increased
chance of having a successful pregnancy.
Please read Dr Vidali’s blog “Silent Endometriosis (diagnosis
based on immune findings without typical symptoms): high incidence in
patients with repetitive IVF failures and Miscarriage” to learn
more on endometriosis and how endometriotic lesions removal could have
beneficial effects on fertility.
As seen in Figure 4, our pregnancy success rates are outstanding in the
younger population categories
who did conceive after therapies under our care, reaching up to 100% of pregnancy success in patients between the age
of 35-37 (p=.0001, a very low p value shows a very high statistical significance).
Patients between 38-40 years old have
88.9% chance of having a successful pregnancy once they conceive under our care
(p=.0001).
The pregnancy success rates remain high in patients aged 41-42 years (75%) or 43 years and older (100%) although the results are not significant due to the low number of patients
in these categories, N= 4 and N=2 respectively.
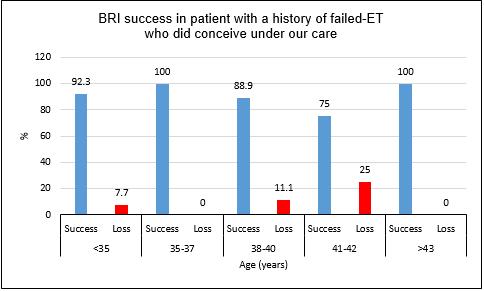
Figure 4: Pregnancy success rate at Braverman Reproductive Immunology based
on patient age with a history of failed-ET prior to our care who conceived
under our care with adequate therapies.
Endometriosis and PCOS (our most common findings)
83.3% of our population with a history of failed-ET prior to coming to
us have been found after our evaluation to have endometriosis and/or PCOS. (Most not knowing they had either until our evaluation) In addition to
immune therapies to counteract inflammation, resection of endometriosis
lesions by our Robotic laparoscopy specialist, and/or adequate therapy
to treat PCOS such as Metformin or the use of our supplement protocol
to help improve mitochondrial function,
92.5% of our endometriosis/PCOS treated patients, who did conceive under
our care, had a successful pregnancy (see Figure 5 (p=.0001).)
The patients in the “other underlying issue category” had other
immune related issues and were treated with aggressive immune therapy.
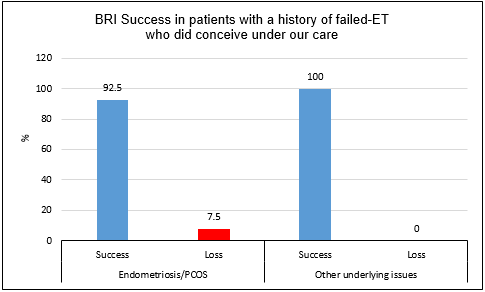
Figure 5: Pregnancy success rate at Braverman Reproductive Immunology based
on patient underlying issues after adequate treatment/surgery and immune
therapies under our care.
Patients with repetitive IVF failures are drained physically, emotionally
and have had a substantial sacrifice on their financial resources. Ultimately
it appears more cost effective to come
Braverman Reproductive Immunology first. We can help you improve your chance of having a healthy pregnancy by identifying
then treating the underlying conditions responsible for your poor egg/embryo
quality or behavior(good quality embryos that do not implant)
We will provide you with the best tailored design strategies to help you
get pregnant and maintain a healthy pregnancy until the delivery of your baby.