Braverman Reproductive Immunology reports Outstanding success rates in women 40-45 years old using their own egg:
Posted By Braverman IVF & Reproductive Immunology || 3-April-2018

Our mitochondrial restoration program for endometriosis appears to overlap and treat age related issues as well!
When looking at our data based on a specific age group at conception, in patients using their own eggs, our success rate is outstanding, reaching over 45% in patients age 40, and up to 37.5% in patients aged 45!
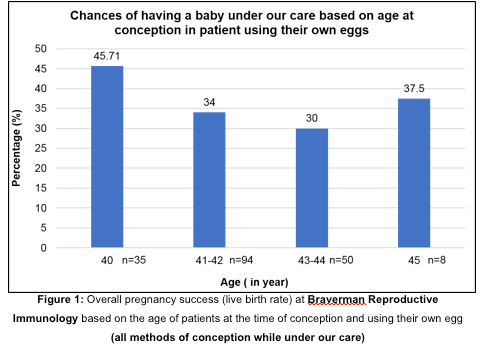
A review of 193 cases at Braverman IVF & Reproductive Immunology
For years we have seen, women, over 40 that come to our practice due to a history of repeated miscarriage or repeated implantation failure, have a significantly higher success rate than what is typically seen in this age group. We decided to focus on this age group (women 40 to 45) and look at our success rates. Fertility in women typically declines with age and decreased success with advancing age has been well documented (1).
We suspect that our high success rates in our patient population aged 40-45 years old is likely due to our program that improves mitochondrial function in the eggs including:
Laparoscopic surgery in women affected by endometriosis and/or peritoneal inflammation.
Immune therapy for those with immune or inflammatory conditions documented by our unique immune profile,
BRAVERMAN REPRODUCTIVE’S ENDO OPTOMIZE SUPPLEMENTS
Our complex patient population is defined as follow:
42 years old on average
3.1 years of infertility
Failed 2.5 IVF cycles prior to our care
experienced more than 2 miscarriages on average prior to our care
78% never had a child prior to our care.
31.6% never got pregnant prior to our care
31% are patients suffering from recurrent pregnancy loss (RPL) with several miscarriages prior to our care ranging from 3 to 9.
1- Our success rates
Reccurent Implantation failure patients
If we look specifically at our patients age 40-45 who were never pregnant prior to our care this represented 31.6 % of our population, and 68.5% conceived using their own eggs, of those almost 40% went on and completed the pregnancy successfully.
Reccurent pregnancy loss patients
If we look at our patients who did conceive prior to our care but who suffered multiple miscarriages (between 3 and 9 prior losses) and representing 31% of our population, 35% of these patients completed a successful pregnancy.
2. At Braverman Reproductive Immunology, our success rates in women aged 40-45 years old are much higher than reported statistics!
Many patients present themselves to Braverman Reproductive Immunology with a history of multiple failed IVF cycles or recurrent pregnancy losses and low AMH levels (AMH < 1). In addition, most also suffer from PCOS and/or endometriosis, both disorders dramatically disrupting egg quality.
When considering our older patient population, you can conclude that they won’t start their fertility journey with the best possible prospects!
In a study (2) reviewing 2,705 in vitro fertilization cycles initiated in women age 40 years and older, for a total of 1263 individual, the overall live birth rate per patient over all cycles was of 20% while our live birth rate in patient regardless of the type of conception was of 34.2% (66/193).
In another study (3) including N=219, 40-year old patients and older, undergoing IVF cycles, the overall live birth rate per patient was 12.3%, our success rate of 34% is almost 3 times higher.
While live birth rate significantly drops to less than 10% at age 43 and older in their study, our success rate remains elevated between 30% (at age 43-44) and 50% (at age 45)!
A low p value as seen by *, **, *** shows that the difference seen is statistically significant.
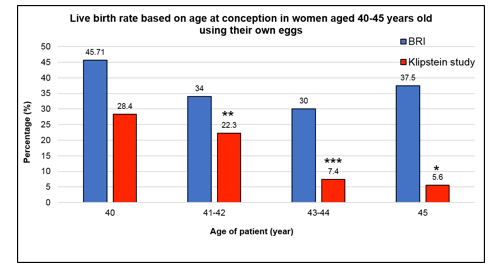
Figure 2: Live birth rate based on patients ‘age at the time of conception and using their own eggs at Braverman Reproductive Immunology in comparison to a reference study
led by Dr Klipstein and collaborators. (* means p value <.05, ** means pvalue <.01, *** means a p value <.001)
If we consider another study (4) where a total of N=30 patients aged 45 underwent a total of 143 IVF cycles, only one in 30 women had a baby so a success rate of 3.33%, way below our 50% success rate in 45-year-old-patient undergoing IVF cycles (Figure 3).
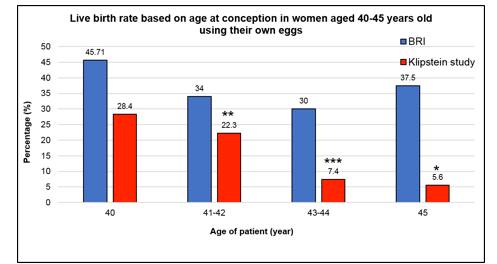
Figure 3: Live birth rate based on patients ‘age at the time of conception and using their own eggs at Braverman Reproductive Immunology in comparison to a reference study led by Dr Tsafrir and collaborators. (* means p value <.05, ** means pvalue <.01, *** means a p value <.001)
In a study (5) presenting the national trends and outcomes of autologous (own egg) in vitro fertilization cycles among women aged 44 years and older, a live birth rate per transfer of 1 to 2% has been reported in cycles resulting in transfers (fresh or frozen). In another report (6), no clinical pregnancies were reported in women aged 45 and no live birth rate was reported in patients aged 44 while our live birth rate per transfer (fresh or frozen) in this patient category reached 16% (8/50) so a rate about 10 times higher!
Strikingly, many of our patients (44/193) will conceive naturally (22.8%) while under our care.
Most surprisingly, almost half of them will get back home with a baby (47.7%) when coming to us!
There are very few studies on natural fertility at advanced age, but one study focused on a community named Hutterites that practices early monogamy and marriage, attempts pregnancy until it is no longer possible, and have strict moral values (no promiscuity, drugs, and alcohol). Their birth rate is very high and 3 times higher than the national average. In this population, one-third of women are infertile by age 40 years and 87% by age 45 (7). Another study, estimates that 63.6% of women who marry between the ages of 40 and 44 years will be at risk for childlessness (8).
This highlights our impressive success rate of 47.7% in older patients that will successfully conceive naturally under our care!
3. Improving your egg quality may help you achieve a successful pregnancy even if you are 40 or older
As women fertility begins to decrease after age 30, delaying childbearing represent a major challenge for fertility treatment. In a large retrospective study (9), a dramatic and significant decrease in embryo implantation rate has been reported with increasing age while all embryos were of similar grade and stage. This decrease has been estimated to 1.5% per year (9).
The decline in fertility in women over 40 is further accentuated. It is caused both by an accelerated follicular loss leading to the reduction of the ovarian reserve (10) and by higher rates of chromosomal abnormalities (aneuploidy) due at least in part to cytoplasmic issues, such as mitochondrial dysfunction (11-12).
These destructive mechanisms linked to ovarian aging but also underlying issues such as PCOS or endometriosis, will ultimately lead to lower pregnancy rates and higher miscarriages.
Although, the studies cited in our blog did not account for the complicated case load that we have here at Braverman Reproductive Immunology, our success rates were significantly higher than those reported in the literature for patients of similar age using autologous oocytes.
How to explain our significantly higher success rates?
As previously reported (13), the number of embryos transferred, significantly influenced the pregnancy success rates so one could argue that we transfer multiple embryos and in fact we generally transfer one to two embryos at most (88% of the time).
Our success may find its roots in our complete program that minimize damage to oocyte (egg) mitochondria and maximize oocyte mitochondrial function. It is important to understand that many areas of treatment are available, and ALL should be employed to make every effort to improve mitochondrial function.
Our comprehensive program does not aim to restore your ovarian reserve to a normal egg count but rather to repair the environment the eggs that are left to develop in, and these eggs can return to developing normally which leads to improved embryo potential and higher chance for a successful pregnancy.
Our protocol includes a support of the ovarian function by using dietary supplements.
We have created a line of dietary supplements Reproductive Immunology Supplements that may help improve mitochondrial function and overall ovarian health.
The line of supplement includes:
Endo-Optimize:
The Endo-Optimize supplement is the result of our work and has been developed to be the best solution to counteract oxidative stress induced-DNA damage and optimize your egg quality as well as minimizing your symptoms associated with endometriosis and PCOS. This “all in one” pill contains many ingredients enhancing mitochondrial activity (a key component in oocyte development) and reducing inflammation thus allowing optimal microenvironment for the oocyte development and maturation.
For more information, read our blog to learn how every ingredients included in our formulation can positively impact your egg quality.
Greens Formula:
Our supplement brings many benefits to your fertility through:
Its hypoglycemic and hypolipidemic potential
Its anti-inflammatory properties
its anti-oxidative properties as one of the most powerful scavenger of free radicals.
For more information, read our blog to learn how our Greens Formula can help improve your fertility.
Omega 3 Optimize:
The latest addition to our supplements is a natural approach to restore optimal fatty acid profile, reduce your inflammation, improve your egg quality and support your pregnancy.
To learn everything you need to know on the benefits omega 3s can have on your fertility, read our blog.
Probiotics
Probiotics are normal inhabitants of the gastrointestinal tract and exert many beneficial effects in a variety of diseases. Taking the right strain at the right dosage could help reduce inflammation among other benefits including:
Anti-inflammatory properties with the reduction of IP-10 levels and other pro-inflammatory cytokines such as IL-17 and interferon-gamma.
Promote immune tolerance by inducing the development of functional regulatory T cells.
Improve insulin sensitivity and glucose metabolism.
Inhibits the development of ectopic endometrial cell in peritoneal cavity (reducing endometriotic lesions).
Besides aging, PCOS and endometriosis are two diseases dramatically impacting your oocyte quality. Adequate care is crucial to improve patients ‘fertility.
To this end and in addition to our dietary supplements, we have developed tailored-design strategies including laparoscopic surgery and immune therapies to counteract any detrimental effects caused by these conditions. To have all the details about our Egg Mitochondrial Restoration Program, consult our blog on the topic.
At Braverman reproductive Immunology, we use a comprehensive and innovative approach that is research-based to maximize your chances of being successful.
We fully understand how mitochondrial dysfunction can affect your fertility, as well as the various ways to treat this condition.
Our diet supplements are available for purchase. For more information about our supplements, please consult our website.
Questions? Call 516.584.8710.
We would be happy to help you take control of your fertility journey and answer any questions you may have.
References
1- CDC. 2016b. Centers for Disease Control and Prevention, American Society for Reproductive Medicine, Society for Assisted Reproductive Technology. 2014 Assisted Reproductive Technology National Summary Report. Atlanta (GA): US Dept of Health and Human Services. https://www.cdc.gov/art/pdf/2014-report/art-2014 national-summary-report.pdf.
2- Klipstein S, Regan M, Ryley DA, Goldman MB, Alper MM, Reindollar RH. One last chance for pregnancy: a review of 2,705 in vitro fertilization cycles initiated in women age 40 years and above. Fertil Steril. 2005;84(2):435–45.
3- Lee Y, Kim TH, Park JK, Eum JH, Lee HJ, Kim J, Lyu SW, Kim YS, Lee WS, Yoon TK. Predictive value of antral follicle count and serum anti-Müllerian hormone: Which is better for live birth prediction in patients aged over 40 with their first IVF treatment? Eur J Obstet Gynecol Reprod Biol. 2018 Feb;221:151-155.
4- Tsafrir A, Simon A, Revel A, Reubinoff B, Lewin A, Laufer N. Retrospective analysis of 1217 IVF cycles in women aged 40 years and older. Reprod BioMed Online. 2007;14(3):348–55.
5- Hipp H, Crawford S, Kawwass JF, Boulet SL, Grainger DA, Kissin DM, Jamieson D. National trends and outcomes of autologous in vitro fertilization cycles among
women ages 40 years and older. J Assist Reprod Genet. 2017 Jul;34(7):885-894.
6- Ron-El R, Raziel A, Strassburger D, Schachter M, Kasterstein E, Friedler S. Outcome of assisted reproductive technology in women over the age of 41. Fertil Steril. 2000 Sep;74(3):471-5.
7- Tietze C. Reproductive span and rate of reproduction among Hutterite women. Fertil Steril 1957;8:89 –97.
8- Menken TJ, Larsen U. Age and infertility. Science 1986;233:1389 –94.
9- Ziebe S, Loft A, Petersen JH et al. 2001 Embryo quality and developmental potential is compromised by age. Acta Obstetricia et Gynecologica Scandinavica 80, 169–174.
10- Faddy, M.J., Gosden, R.G., Gougeon, A., Richardson, S.J., Nelson, J.F., 1992. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum. Reprod.
7, 1342– 1346.
11- Hassold, T., Hunt, P., 2009. Maternal age and chromosomally abnormal pregnancies: what we know and what we wish we knew. Curr. Opin. Pediatr. 21, 703–708.
12- Miao, Y.-L., Kikuchi, K., Sun, Q.-Y., Schatten, H., 2009. Oocyte ageing: cellular and molecular changes, developmental potential and reversal possibility. Hum. Reprod. Update 15, 573–585.
13- Opsahl MS, Blauer KL, Black SH et al. 2001 The number of embryos available for transfer predicts successful pregnancy outcome in women over 39 years with normal ovarian hormonal reserve testing. Journal of Assisted Reproduction and Genetics 18, 551–556.